Get Ps 18 Form in PDF
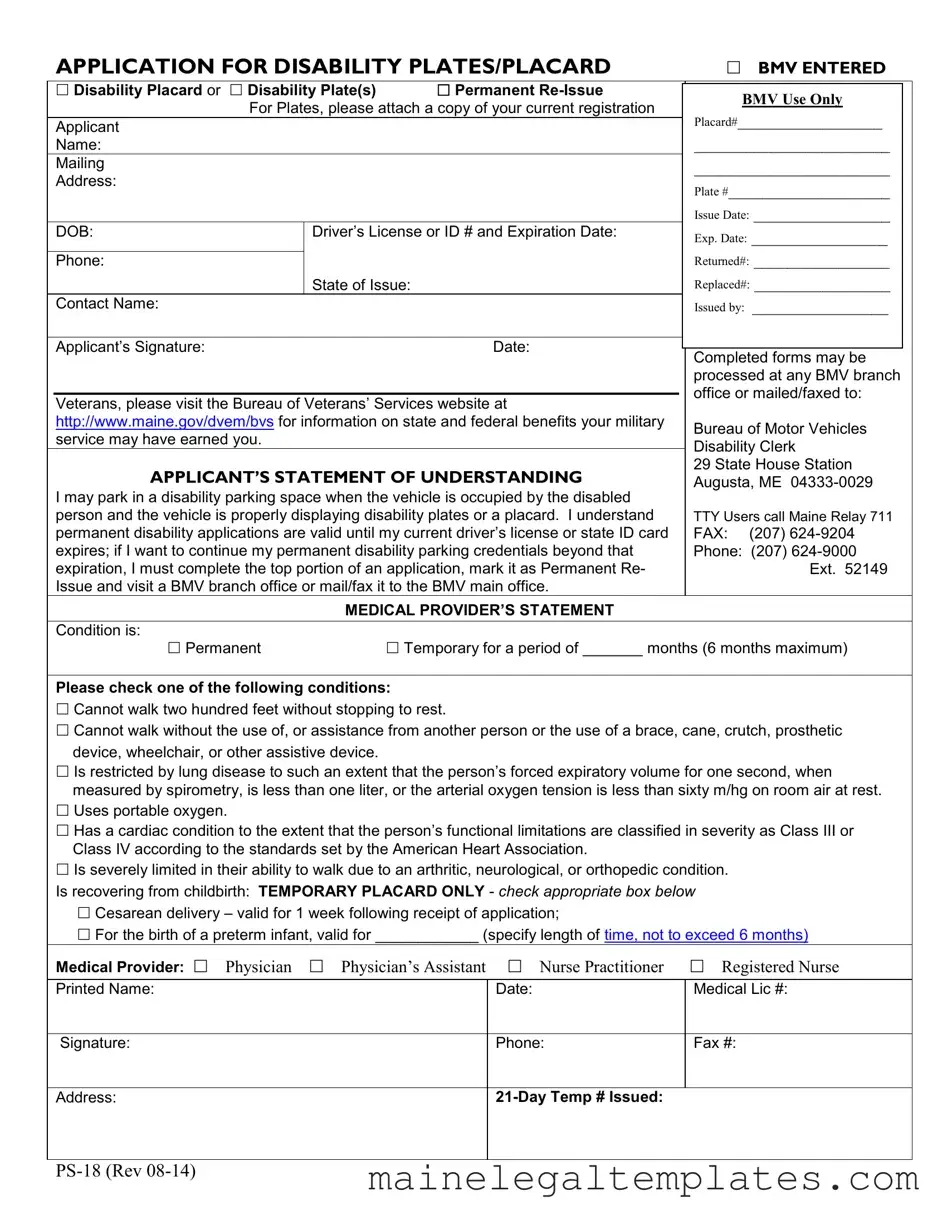
The Ps 18 form serves as a crucial application for individuals seeking disability plates or placards in the United States. This form is designed to facilitate access to designated parking spaces for those with mobility challenges. It allows applicants to request either a disability placard or disability plates, ensuring that they can park in areas specifically reserved for their needs. The application requires personal information, including the applicant's name, address, and driver's license details, to verify eligibility. Additionally, it includes a statement of understanding, where applicants acknowledge the rules surrounding the use of disability parking spaces. A medical provider's statement is also a vital component, confirming the applicant's condition and its impact on mobility. The form outlines various qualifying conditions, ranging from temporary limitations due to childbirth to permanent disabilities. This comprehensive approach ensures that those who truly need assistance can obtain the necessary credentials to make their daily lives more manageable. By understanding the Ps 18 form and its requirements, applicants can navigate the process with confidence, knowing that their needs will be met with the appropriate accommodations.
Dos and Don'ts
When filling out the Ps 18 form, there are important guidelines to follow. Here’s a list of what you should and shouldn’t do:
- Do provide accurate personal information, including your name and address.
- Do ensure that your medical provider signs and dates the application.
- Do attach a copy of your current vehicle registration if applying for a disability plate.
- Do check the box that accurately describes your condition.
- Don't leave any required fields blank; incomplete forms may delay processing.
- Don't forget to specify if your condition is temporary or permanent.
- Don't submit the form without reviewing it for errors.
- Don't forget to keep a copy of the completed form for your records.
Key takeaways
When filling out the Ps 18 form for disability plates or placards, keep these key takeaways in mind:
- Eligibility Requirements: Ensure that you meet the criteria for disability parking. This includes having a permanent or temporary condition that significantly limits mobility.
- Accurate Information: Fill in all required fields accurately, including your name, address, and medical condition. Incomplete forms may delay processing.
- Medical Provider's Verification: Obtain a signature from a qualified medical provider. This could be a physician, physician’s assistant, or nurse practitioner who can confirm your disability.
- Temporary vs. Permanent: Clearly indicate whether you are applying for a permanent or temporary placard. Temporary placards are valid for a limited time and must be renewed.
- Submission Options: Completed forms can be submitted in person at any BMV branch office or sent by mail or fax to the main office. Choose the method that works best for you.
- Renewal Process: If you have a permanent disability placard, remember that it remains valid until your driver’s license or state ID expires. To continue using it, you must reapply before expiration.
- Parking Regulations: Understand the rules for using disability parking spaces. You can park in these spaces only when the vehicle is occupied by the person with the disability and properly displaying the placard or plates.
Instructions on Filling in Ps 18
Filling out the PS 18 form is a straightforward process. It requires specific information about the applicant and their medical condition. Make sure to gather all necessary documents before you begin. Once completed, the form can be submitted in person at any BMV branch office or sent by mail or fax to the designated address.
- Begin by selecting the type of application: Disability Placard or Disability Plate(s). If you are reapplying, mark Permanent Re-Issue.
- In the provided space, write your Applicant Name.
- Fill in your Mailing Address.
- If applying for plates, attach a copy of your current registration and write your Plate # and Issue Date.
- Enter your Date of Birth (DOB).
- Provide your Driver’s License or ID # and its Expiration Date.
- List your Phone number.
- Indicate the State of Issue for your ID.
- Fill in any Returned# or Replaced# if applicable.
- Provide the Contact Name for further correspondence.
- Write the name of the individual or organization that Issued the application.
- Sign and date the form in the Applicant’s Signature section.
- Review the Applicant’s Statement of Understanding and ensure you understand the conditions for using disability parking.
- In the Medical Provider’s Statement, check whether your condition is Permanent or Temporary, and specify the duration if temporary.
- Check the appropriate box that describes your condition from the list provided.
- If applicable, fill in details regarding recovery from childbirth for a temporary placard.
- Provide the Medical Provider details, including their printed name, medical license number, signature, phone, and fax number.
- Write the Address of the medical provider.
- If you have a 21-Day Temp # issued, include that number.
Find Popular Forms
Maine Advance Directive Form - An agent can't be a staff member of a facility where you receive care, unless they are related to you.
When engaging in the purchase or sale of an ATV in New York, it is crucial to utilize a proper legal document to safeguard both parties involved. The New York ATV Bill of Sale form not only serves as proof of transaction but also aids in the registration process under the new owner's name. For a reliable template to create this important document, you can visit nyforms.com/atv-bill-of-sale-template/.
Afppgmc Updating Skype - All applications are subject to verification against provided documentation.
Learn More on This Form
-
What is the Ps 18 form?
The Ps 18 form is an application for disability plates or placards issued by the Bureau of Motor Vehicles (BMV). It allows individuals with disabilities to obtain special parking privileges by displaying a disability plate or placard on their vehicle. This form is essential for those who qualify for these benefits under state regulations.
-
Who is eligible to apply for a disability placard or plate?
Eligibility for a disability placard or plate generally includes individuals who cannot walk without assistance or have a medical condition that severely limits their mobility. Specific criteria include those who:
- Cannot walk two hundred feet without stopping to rest.
- Require assistance from another person or an assistive device.
- Have significant lung disease or cardiac conditions as defined by medical standards.
- Are recovering from childbirth (temporary placard only).
-
How do I complete the Ps 18 form?
To complete the Ps 18 form, you will need to provide personal information such as your name, address, date of birth, and driver’s license number. Additionally, a medical provider must certify your condition by completing their section of the form. Be sure to check whether you are applying for a permanent or temporary placard, as this will affect the details you need to provide.
-
Where can I submit the completed Ps 18 form?
You can submit the completed form at any BMV branch office. Alternatively, you may choose to mail or fax it to the BMV main office. Ensure that all required information is filled out correctly to avoid delays in processing your application.
-
What should I do if my disability parking credentials expire?
If your disability parking credentials are set to expire, you must complete the top portion of a new application and mark it as “Permanent Re-Issue.” This process must be done before your current credentials expire to ensure that you maintain your parking privileges.
-
How long is a temporary disability placard valid?
A temporary disability placard is typically valid for a maximum of six months. The exact duration will depend on the medical condition specified by your healthcare provider. For instance, if you are recovering from childbirth, the placard may be valid for one week or a specific period as indicated by your medical provider.
-
What should I do if I have questions about my application?
If you have questions regarding your application or need assistance, you can contact the BMV directly. They can provide guidance and clarify any uncertainties about the application process, eligibility, or required documentation. You can reach them via phone or visit their website for more information.
File Attributes
| Fact Name | Details |
|---|---|
| Form Purpose | This form is used to apply for disability plates or placards in Maine. |
| Eligibility Criteria | Applicants must have a permanent or temporary disability that limits mobility. |
| Application Submission | Completed forms can be submitted at any Bureau of Motor Vehicles (BMV) branch or mailed/faxed to the main office. |
| Medical Provider Requirement | A medical provider must certify the applicant's disability on the form. |
| Temporary Placard Validity | Temporary placards are valid for a maximum of 6 months, depending on the condition. |
| Permanent Re-Issue | To maintain permanent disability credentials, applicants must reapply before their driver's license expires. |
| Contact Information | Applicants can reach the BMV at (207) 624-9000 for assistance. |
| Governing Law | This form is governed by Maine state law regarding disability parking permits. |
Documents used along the form
When applying for disability plates or placards, several additional forms and documents may be necessary to ensure a smooth and efficient process. Each of these documents serves a specific purpose, providing vital information that supports the application. Below is a list of commonly used forms that may accompany the Ps 18 form.
- Medical Provider’s Statement: This document must be completed by a qualified medical professional. It verifies the applicant's disability and specifies whether the condition is permanent or temporary. The statement includes details about the applicant's mobility limitations and may require the provider's signature and contact information.
- Application for Temporary Disability Placard: This form is specifically for individuals who require temporary disability parking privileges. It outlines the conditions under which the temporary placard is issued and includes a defined validity period, typically not exceeding six months.
- Proof of Residency: Applicants may need to submit documentation that confirms their residency in the state. This could include a utility bill, lease agreement, or any official correspondence that clearly states the applicant's name and address.
- Washington Articles of Incorporation Form: To properly establish your business in the state, refer to the complete Washington Articles of Incorporation form guide for necessary steps and documentation.
- Identification Documentation: A copy of the applicant’s driver’s license or state ID is often required. This helps verify the identity of the applicant and ensures that the disability plates or placards are issued to the correct individual.
- Application for Renewal: For those seeking to renew their disability plates or placards, a renewal application form may be necessary. This document typically requires the same information as the initial application, along with any updates regarding the applicant’s medical condition.
- Affidavit of Disability: In some cases, an affidavit may be required to affirm the applicant's disability status. This sworn statement can provide additional legal backing for the application and may be used to clarify any ambiguities regarding the applicant’s eligibility.
- Authorization for Release of Medical Information: This form allows the applicant to authorize their medical provider to share relevant health information with the Bureau of Motor Vehicles. It ensures that the BMV has access to necessary medical documentation to process the disability application effectively.
Each of these documents plays a crucial role in the application process for disability plates or placards. By ensuring that all necessary forms are completed and submitted, applicants can facilitate a more efficient review and approval process. Understanding the requirements and preparing the appropriate documentation can significantly ease the journey toward obtaining the needed accommodations.
Misconceptions
Misconceptions about the PS 18 form can lead to confusion for applicants seeking disability plates or placards. Here are nine common misunderstandings:
- Only individuals with permanent disabilities can apply. Many believe that only those with permanent disabilities are eligible for disability plates or placards. In reality, the form accommodates both permanent and temporary disabilities, allowing for a range of conditions.
- The application must be submitted in person. Some think that they must visit a Bureau of Motor Vehicles (BMV) office to submit their application. However, the PS 18 form can also be mailed or faxed to the BMV, providing more flexibility for applicants.
- Disability plates and placards are the same. Many people assume that disability plates and placards serve the same purpose. While both allow for parking in designated spaces, plates are attached to the vehicle, whereas placards are portable and can be used in different vehicles.
- Only medical professionals can fill out the form. There is a misconception that only licensed medical providers can complete the necessary medical statements. In fact, applicants can provide personal information and have their medical provider fill out the relevant sections.
- Once issued, the placard or plate is permanent. Some individuals believe that once they receive their disability placard or plate, it will last indefinitely. In truth, permanent disability applications are valid only until the expiration of the applicant’s driver’s license or state ID card. Renewal is required to maintain eligibility.
- Temporary placards are only for new mothers. While it is true that temporary placards can be issued for childbirth, they are also available for other temporary conditions. Applicants with temporary disabilities lasting up to six months can apply for these placards.
- All disabilities are automatically accepted. There is a belief that any claimed disability will qualify for a placard or plate. However, specific criteria must be met, and medical documentation is required to validate the application.
- There is no need for a medical provider’s signature. Some applicants think they can submit the form without a medical provider’s endorsement. A signature from a qualified medical professional is essential for verifying the disability.
- Applicants must pay a fee for the placard or plate. Many assume there is a cost associated with obtaining disability plates or placards. In fact, these are typically issued at no charge, making them accessible for those in need.
Understanding these misconceptions can help individuals navigate the application process more effectively and ensure they receive the appropriate accommodations for their disabilities.
Document Preview
|
APPLICATION FOR DISABILITY PLATES/PLACARD |
|
BMV ENTERED |
|||||
|
|
|
|
|
|
|
|
|
|
Disability Placard or Disability Plate(s) |
Permanent |
|
|
|
|
||
|
|
BMV Use Only |
|
|||||
|
For Plates, please attach a copy of your current registration |
|
|
|||||
|
|
Placard#_________________ |
|
|||||
|
Applicant |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
Name: |
|
|
|
|
_______________________ |
|
|
|
Mailing |
|
|
|
|
_______________________ |
|
|
|
Address: |
|
|
|
|
Plate #___________________ |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
Issue Date: ________________ |
|
|
|
DOB: |
Driver’s License or ID # and Expiration Date: |
|
Exp. Date: ________________ |
|
|||
|
|
|
|
|
|
|
||
|
|
|
|
|
|
Returned#: ________________ |
|
|
|
Phone: |
|
|
|
|
|
||
|
|
State of Issue: |
|
Replaced#: ________________ |
|
|||
|
Contact Name: |
|
|
|
|
Issued by: ________________ |
|
|
|
|
|
|
|
|
|
|
|
|
Applicant’s Signature: |
|
Date: |
|
|
|
|
|
|
|
|
Completed forms may be |
|||||
|
|
|
|
|
|
|||
|
|
|
|
|
|
processed at any BMV branch |
||
|
|
|
|
|
|
office or mailed/faxed to: |
||
|
Veterans, please visit the Bureau of Veterans’ Services website at |
|||||||
|
|
|
|
|||||
|
http://www.maine.gov/dvem/bvs for information on state and federal benefits your military |
Bureau of Motor Vehicles |
||||||
|
service may have earned you. |
|
|
|
|
|||
|
|
|
|
|
Disability Clerk |
|||
|
|
|
|
|
|
|||
|
APPLICANT’S STATEMENT OF UNDERSTANDING |
29 State House Station |
||||||
|
Augusta, ME |
|||||||
|
|
|
|
|
|
|||
|
I may park in a disability parking space when the vehicle is occupied by the disabled |
|
|
|
||||
|
person and the vehicle is properly displaying disability plates or a placard. I understand |
TTY Users call Maine Relay 711 |
||||||
|
permanent disability applications are valid until my current driver’s license or state ID card |
FAX: |
(207) |
|
||||
|
expires; if I want to continue my permanent disability parking credentials beyond that |
Phone: |
(207) |
|
||||
|
expiration, I must complete the top portion of an application, mark it as Permanent Re- |
|
Ext. 52149 |
|||||
|
Issue and visit a BMV branch office or mail/fax it to the BMV main office. |
|
|
|
||||
|
|
MEDICAL PROVIDER’S STATEMENT |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
Condition is: |
|
|
|
|
|
|
|
|
Permanent |
|
Temporary for a period of _______ months (6 months maximum) |
|||||
Please check one of the following conditions:
Cannot walk two hundred feet without stopping to rest.
Cannot walk without the use of, or assistance from another person or the use of a brace, cane, crutch, prosthetic device, wheelchair, or other assistive device.
Is restricted by lung disease to such an extent that the person’s forced expiratory volume for one second, when measured by spirometry, is less than one liter, or the arterial oxygen tension is less than sixty m/hg on room air at rest.
Uses portable oxygen.
Has a cardiac condition to the extent that the person’s functional limitations are classified in severity as Class III or Class IV according to the standards set by the American Heart Association.
Is severely limited in their ability to walk due to an arthritic, neurological, or orthopedic condition. Is recovering from childbirth: TEMPORARY PLACARD ONLY - check appropriate box below
Cesarean delivery – valid for 1 week following receipt of application;
For the birth of a preterm infant, valid for ____________ (specify length of time, not to exceed 6 months)
Medical Provider: Physician Physician’s Assistant |
Nurse Practitioner |
Registered Nurse |
|
|
|
Printed Name: |
Date: |
Medical Lic #: |
|
|
|
Signature: |
Phone: |
Fax #: |
|
|
|
Address: |
|
|
|
|
|